Volume 9, Issue 5 - May 2026
|
The Conscience of a Professional: Employers, Environment, and Emotions
By: Bryan Pilkington, PhD
|

The May issue of The Academy precedes APHC’s major gathering, the June Conference. This year’s conference, Professionalism and Advocacy: Achievements, Barriers, Complexities takes place from June 3rd to 5th at Cooper Medical School of Rowan University (CMSRU) in Camden, NJ. The conference promises to be a home for important healthcare professionalism conversations. It is a hybrid conference, so do consider attending virtually if you are unable to be there in person. This month’s issue also precedes an excellent round table discussion taking place on Friday, May 8th, at 3:00 PM; Drs. Joshua Owolabi and Mohamud Verjee will discuss their article “Professionalism in Scholarship Leadership.” While the May issue customarily highlights exciting talks at the conference or piques the reader’s interest in May’s roundtable topic, we’ll save both for our June issue – and do a deep dive, post mortem on the conference and roundtable. Instead, this issue focuses on three timely topics in healthcare professionalism all of which are sure to be touched on at the conference – both in sessions and by the proverbial watercooler (read: main zoom room or coffee break table).
In our lead article, Thomas Harter, former President of the APHC, brings together two seemingly separate topics – conscientious objection and artificial intelligence – to reflect on the future of healthcare professionalism. This is a power – and provocative! – piece that pushes those who work on healthcare professionalism, who teach professional identity formation in health professions training institutions, as well as those interested in the role of AI in healthcare and its impact on healthcare professionals.
With Earth Day being celebrated recently, the impact of climate change on health is on the minds of many. In our second article, Hajrah Hussain argues that health professionals have a professionalism-based obligation to advocate for the protection of the environment. Hussain relies on a case study – physicians in New Jersey – to make her argument, doing so in a way that is generalizable beyond the locale which she focuses on. From concerns about medical waste to the harmful environmental effects of the overuse of AI by health systems, healthcare professionals need to think about the demands for advocacy on behalf of their patients. Hussain’s work will help us all do that better.
In our final article, Jenna Mustafa picks up on themes discussed in the last issue of The Academy involving shame and medicine. In that issue, Will Bynam, Luna Dolezal, Gioconda Mojica, Angelo Cadiente, and Jamie Chen discussed – from different professional perspectives - the importance of considering shame in healthcare interactions and training. Mustafa extends that conversation. She departs from some philosophical accounts of shame and considers it primarily as an emotion, focusing on the plight of some medical trainees, given systems that are in drastic need of a professionalism-based reworking.
Taken together, these three articles are an excellent lead into the conversations that are to be housed in the June conference. Taking the demands of healthcare professionalism seriously might mean advocating for better climate-related practices, more cognizantly attending to the shame felt by trainees, and continuing discussions about the role of conscience in healthcare. Personally, I look forward to learning more from all of you on each of these important topics in June.
And be sure to check out the member announcements and accomplishments area and information about registering for the conference.
Bryan Pilkington, PhD, is Professor of Bioethics, in the Department of Medical Sciences, at Hackensack Meridian School of Medicine, and the Editor-in-Chief of The Academy: A Forum for Conversations about Health Care Professionalism.
|
|
Join a global community of healthcare professionals at this year’s Hybrid International Conference, hosted in person at Cooper Medical School of Rowan University in Camden, NJ, and virtually via Zoom.
The conference features 60+ hybrid sessions, including keynote presentations, workshops, panels, symposia, oral and flash presentations—all recorded for on-demand access.
Explore timely topics such as advocacy in healthcare, self-advocacy and wellness, interprofessional teamwork, global perspectives, ethical responsibilities, and effective advocacy training.
🎓 Attend in person or online and be part of the conversation shaping the future of professionalism and advocacy in health care.
👉 Click here to for more info
👉 Click here for the schedule
👉 Click here to register
👉 Click here for nearby hotels
Back to Table of Contents
|
|
|
Healthcare Professionalism’s Approaching Identity Crisis: Is It Time to Start Saying the Quiet Parts Out Loud?
By: Thomas Harter, PhD
|
This article addresses two ideas that seem unrelated to one another but are – in my estimation – deeply connected and, together, represent an important reality in the field of healthcare professionalism, one which we need to contend with in ways that may be uncomfortable for many physicians and other health care professionals. Conscientious objection and artificial intelligence (AI) – and the vast number of articles written and personal reactions individuals have to both – are, admittedly, strange bedfellows, but bedfellows nonetheless. Their connection to health care is the result of deeply embedded values that guide ideal healthcare professionalism. While this short piece is likely to provoke strong emotions and reactions, my intention is only to note that there is no utopian notion of healthcare professionalism and to begin a dialogue about what it means – or will mean – to be a healthcare professional in the wake of AI’s rapid incorporation in all aspects of health care.
Medical ethics is rooted in the concept of respect for patient autonomy. Conscientious objection – stemming from the idea that respect for autonomy also applies to healthcare professionals – supports the right of healthcare professionals to refuse legally sanctioned treatments requested by patients that healthcare professionals have a personal moral or religious opposition to. In the realm of medical ethics, conscientious objections are considered ethically problematic for numerous reasons but primarily because they thwart patient access to otherwise legally entitled health care and potentially subject patients to medically paternalistic biases, value judgments, and shame. One way to view the idea of conscientious objections in health care, however, is that it is a consequence of training healthcare professionals not to be mindless worker bees simply acquiescing to the demands of patients, but to be thoughtful, reflective, caring individuals – a primary goal of healthcare professionalism and professional identity formation education.
The use of AI in healthcare is regularly criticized for two reasons. First, its adoption in patient care is happening too fast to carefully identify and navigate the potential negative effects it might have (or is already having) on patient care, such as exacerbating underlying inequalities in health care delivery among diverse populations. Second, AI is impersonal and lacks an essential – yet ill-defined – humanistic quality that exists only in person-to-person, provider-to-patient interactions. Tied to these two problems is an often-expressed underlying fear that AI makes – or will make – many of the tasks and functions of various healthcare professions automated in ways that make the use of human healthcare providers redundant and unnecessary.
Yet the rise of AI in health care has been brewing for decades. As new medical advances and the influences of politics, law and economic pressures increase the complexity of patient care, healthcare professionals have been forced to divert their attention away from practicing patient care toward managing those pressures. A relatively common contemporary complaint by healthcare professionals is that they spend too much time during patient care appointments documenting their conversations with patients and not enough time being mindfully present and engaged in those conversations. AI offers the possibility to relieve some (perhaps many) of the various pressures that divert healthcare professionals’ attention away from their patients. One example is the use of ambient, conversational AI to listen to patient-provider conversations, summarize them, and assimilate them into correct medical records documentation, freeing healthcare professionals to refocus on being engaged with their patients during appointments rather than typing on a keyboard. AI is also objective and does not (yet) have moral reasoning to influence its assessments of diagnostic or treatment recommendations for patients. This means that AI – should it develop to the degree of helping manage patient care – has the potential to eliminate the various and numerous biases and value judgements that lead to explicit and implicit discrimination in the delivery of health care (rather than exacerbate it). In short, AI can be a tool of just healthcare, not its antithesis.
Why does all this matter? The field of healthcare professionalism is facing a potential identity crisis. Humans are complex, dynamic, rationally and emotionally clumsy creatures. For all the compassion and empathy health care professionals can express in the care of others, they are also flawed and can harm patients in terms of unjust discrimination and bias. AI is impersonal, inherently lacking an important quality of humanism. Yet, its potential for objective assessment, data analysis, and diagnostic capacity, may be the course correction medical ethics and the field of healthcare professionalism have been looking for in terms of just, high-quality patient care. In the very near future, health care professionals – and those working and educating in the healthcare professionalism space – will therefore need to decide what values really matter most in terms of education and patient care and what trade-offs we as educators, healthcare providers, and patients are willing to accept in the delivery of healthcare. Are we willing to trade-off the ethical and moral conflicts that arise when provider values clash with patients, such as what happens with conscientious objections, for more precise, value-neutral care delivered robotically or will we continue to prefer care delivered by humans even in the face of missed diagnoses, delayed care, unrelenting distractions, and values clashes and dilemmas at the center of conscientious objections?
Thomas D. Harter is the Director of Bioethics and Humanities with Emplify Health by Gundersen. He is a former president of the Academy for Professionalism in Health Care and is the co-editor of the recently published textbook, Medical Professionalism: Theory, Education and Practice.
Back to Table of Contents
|
The Physician’s Professional Responsibility to Advocate for Environmental Protection
By: Hajrah Hussain
|
Physicians can treat patients with asthma in their clinics but when communities are disproportionately impacted with higher rates of asthma is there a role for physician advocacy outside of the clinic? This paper serves to explore the role of physician advocacy using the case study of a proposed fourth power plant in Newark, NJ. A parallel can be drawn between trauma surgeons advocating for firearm violence prevention upstream of the bullets they extract from patients and primary care physicians and pulmonologists advocating for stricter air quality regulations to prevent asthma exacerbations. The American Lung Association documents the connection between air pollution and asthma but demonstrating that connection for patient education instead of regulatory advocacy places the onus on individuals instead of systems (ALA, 2025).
Environmental justice is defined by the Environmental Protection Agency (EPA) as “the fair treatment and meaningful involvement of all people regardless of race, color, national origin, or income with respect to the development, implementation and enforcement of environmental laws, regulations, and policies.” New Jersey’s Environmental Justice Law passed in 2020 was heralded as a win for historically overburdened communities as it requires the NJ Department of Environmental Protection “to evaluate environmental and public health impacts of certain facilities on overburdened communities (OBCs) when reviewing certain applications. NJ is the first state required to issue denials for new facilities that cannot avoid disproportionate impact on OBCs or serve compelling public interest.” This new law was put to the test with the Passaic Valley Sewerage Commission (PVSC) proposal to build a fourth natural gas power plant in Newark, NJ.
Since 2021, PVSC’s board of commissioners monthly meetings have been attended by community advocates from across New Jersey stating that the addition of a fourth natural gas power plant in Newark, NJ should not be allowed as the community qualifies as an OBC that would be harmed with this new construction. PVSC maintains the necessity of a fourth power plant for their sewage operations by citing the outage they experienced during Superstorm Sandy and the need for additional power in the event of a future climate event like Sandy (Tobia, 2025). Citing an environmental event to justify a construction that would perpetuate negative environmental effects daily rings hollow. Newark has three times the state average of pediatric asthma rates with 1 in 4 children affected (EPA, 2016). Newark also averaged one child death from asthma from 2010 - 2017 per the NJ Department of Health (Bose, 2019). Given that asthma is a treatable condition but social determinants of health, such as access, can still lead to mortality, it is all the more important to assess upstream solutions.
Physicians in advocacy spaces aiming to affect regulatory changes are often told to “stay in their lane” but when their lane includes the treatment of preventable conditions it can also include their prevention. Advocacy is an element of professionalism that can ensure physicians as professionals are grounded in their communities. Even the treatment of asthma is not without environmental implications given that 90% of patients with asthma in the US use metered dose inhalers containing hydrofluoroalkanes with carbon emissions comparable to 550,000 cars annually (Feldman & Furie, 2025). While changes in prescribing practices can run into obstacles in the health insurance space in terms of what insurers provide coverage for, there are many inroads to addressing asthma and air pollution such as advocating for stronger regulations of air pollution.
Returning to the case study of PVSC, their board of commissioners approved the fourth power plant this past spring despite four years of community advocacy. In October 2025, Earthjustice filed a petition against PVSC on behalf of Ironbound Community Corps, the organization that had facilitated community representation over the years, stating that the construction violates the NJ Environmental Justice Law’s protection of overburdened communities. That same month Mayor Ras Baraka and the City of Newark filed their own lawsuit against PVSC as well. These lawsuits would be well-supported by physician testimonies as expert witnesses regarding the pediatric asthma rates and deaths in Newark.
REFERENCES
Association, A. L. (2025). Understanding the strong link between air pollution and Asthma. American Lung Association. https://www.lung.org/blog/asthma-and-air-pollution
Environmental Protection Agency. (2016, September 23). Community Air Monitoring where you live in EPA region 2. EPA. https://19january2017snapshot.epa.gov/air-sensor-toolbox/ community-air-monitoring-where-you-live-epa-region-2_.html
Environmental Protection Agency. (2020, September 24). Learn about environmental justice. EPA. https://19january2021snapshot.epa.gov/environmentaljustice/learn-about-environmental-justice_.htmlhttps://19january2021snapshot.epa.gov/environmentaljustice/learn-about-environmental-justice_.html
Feldman, W. B., & Furie, G. (2025). The moral injury of Inhaler prescribing. New England Journal of Medicine, 392(9), 836–839. https://doi.org/10.1056/nejmp2412383
Fitzgerald, E. (2025, October 27). NJ Court prohibits construction of controversial Newark Gas Plant. Earthjustice. https://earthjustice.org/press/2025/nj-court-prohibits-construction-of-controversial-newark-gas-plant
Hamilton, D. (2024). ACS commends U.S. Surgeon General’s advisory on Firearm Violence. ACS. https://www.facs.org/media-center/press-releases/2024/acs-commends-us-surgeon-generals-advisory-on-firearm-violence/
Tobia, D. (2025, November 25). Proposed Ironbound Power Plant Faces legal pushback from Newark and community groups. Jersey Digs. https://jerseydigs.com/pvsc-power-plant-newark/
Hajrah Hussain is a medical student interested in the social determinants of health including the built environment and the disproportionate effects of pollution on working-class communities of color.
Back to Table of Contents
|
Shame and Medicine as it Pertains to the Medical Trainee
By: Jenna Mustafa
|
Medicine is an intense field of practice, with momentous, life-or-death situations occurring daily. Training in such an environment can be an exhilarating, wondrous experience. Learning through patient interaction is a pivotal element of medical education. Students are paired with senior staff, and taught through hands-on experience. While this is a great way to learn, students are more prone to mistakes. Unfortunately, shame can creep into the picture when dealing with high-stakes scenarios. Many trainees echo that their clinical years exponentially enhanced their learning, but most also have experienced significant shame throughout their learning, especially as early trainees. Shame is often defined as a state of negative perception of one-self characterized by inadequacy, or low self-worth, among other negative emotions.1
Medical students are especially vulnerable throughout their educational timelines. That shame may come from anyone, often from superiors in their own profession, superiors in neighboring professions, or the patient themselves. Recently, shaming medical students has become common on social media as well. Up to 90% of medical students report feeling humiliation at some point during their training2, a harrowing number considering this is after many efforts have been made to prioritize inclusion in medical education. With shame coming from all directions, students often feel isolated and alone. This shame often takes place in inescapable encounters. For example, inside of an operating room during surgery, in a patient room during an encounter, or on morning rounds with a full team. 80% of surveyed medical students reported feeling at least partially fearful when questioned on ward rounds, with 60% reporting shame specifically.3
Shame can have a profoundly negative impact on student mental health and wellbeing, combining both emotional and physical distress4. Students often reported an acute phase of shame, with a brisk emotional upswell that triggered physical sensations of panic (flushing, retreating, etc.). Students exhibited both rumination and flashbacks to events where they were severely humiliated. Many students reported chronic shame that followed them throughout their time in medical school. Chronic shame can lead to significant adverse health outcomes, namely depression, addiction, eating disorders, anxiety, and rage responses, among many other psychosocial distressors.
Medical schooling often integrates a Professionalism grade into a student’s final grade. While professionalism is not easy to describe, it is an understandable part of medical education. Quantitative measures (the number of times a student may be late, miss an assignment, etc.) are an easy way to record this grade. However, how does one quantify a student’s professionalism through behavior and patient interaction? Medicine is often criticized for its “hidden curriculum5,” or the behaviors and values transmitted to students beyond official lessons. The ambiguous nature of the Professionalism grade allows for perpetuation of said “hidden curriculum,” as a student may never know what can be factored into this aspect of their grade. Therefore, a student may undergo significant shaming, especially during clinical training, without reporting this negative behavior to appropriate parties. This may be for a number of reasons, but fear of retaliation is often a large contributing factor. One study found that in assessing reasons why students did not report mistreatment, fear of reprisal was the second most common factor6. Whether out of concern that their superiors could negatively impact their grades, or fear of “burning bridges” in the future, students were hesitant to report mistreatment. The availability of anonymous reporting systems did not significantly change this hesitancy. Specialty-concordant fear of retaliation was especially prominent.
Some proposed solutions to address shame in medical education include faculty development focused on constructive feedback, formal anti-mistreatment policies, and established mentorship systems for immediate avenues of support. Training for medical educators should include differentiating between rigorous teaching and humiliation, emphasizing that degradation has no place in healthy learning. Studies suggest that supportive learning environments are associated with lower levels of burnout, less career regret, and improved empathy in students7. Confidential, accessible, and regularly accessed reporting systems should be commonplace in learning institutions. Furthermore, seeing actual action resulting from valid complaints increases trust in the reporting process. Additionally, reevaluating vague professionalism metrics and replacing them with clear, behavior-based standards may reduce opportunities for bias and misuse of power8,9.
In conclusion, shame is a powerful emotion that exists heavily among medical students during training. It can negatively impact a student’s health for life. Students often experience humiliation, but under-report these instances for a variety of reasons, but most notably out of fear of retaliation for their grades or future careers. Ultimately, medicine must recognize that shame is not an educational tool but a barrier to growth. A culture that emphasizes accountability, psychological safety, and respect will better protect trainee wellbeing while producing more confident, compassionate physicians. The medical community must come together to create a safe learning environment for trainees, minimizing shame and prioritizing student wellbeing and educational gain.
REFERENCES
- Laura Weiss Roberts, Addressing Shame in Medical Education, Academic Medicine, Volume 98, Issue 6, June 2023, Pages 649–650, https://doi.org/10.1097/ACM.0000000000005209
- Wigg, L., Li, W.W. & Leow, T. A Systematic Review and Meta-analysis on Teaching by Humiliation in Medical Training: Its Frequency and Impact on the Mental Health Outcomes of Medical Trainees. Med.Sci.Educ. 35, 569–585 (2025). https://doi.org/10.1007/s40670-024-02213-7
- Barry K, Schiffman FJ, Collins BJ. Assessing Medical Student Fear and Shame as Barriers to Active Participation on the Wards. Brown Hospital Medicine. 2022;2(1). doi:10.56305/001c.40087. PMID:40046546
- Bynum WE 4th, W Teunissen P, Varpio L. In the "Shadow of Shame": A Phenomenological Exploration of the Nature of Shame Experiences in Medical Students. Acad Med. 2021;96(11S):S23-S30. doi:10.1097/ACM.0000000000004261
- Lawrence C, Mhlaba T, Stewart KA, Moletsane R, Gaede B, Moshabela M. The Hidden Curricula of Medical Education: A Scoping Review. Acad Med. 2018;93(4):648-656. doi:10.1097/ACM.0000000000002004
- Chung MP, Thang CK, Vermillion M, Fried JM, Uijtdehaage S. Exploring medical students' barriers to reporting mistreatment during clerkships: a qualitative study. Med Educ Online. 2018;23(1):1478170. doi:10.1080/10872981.2018.1478170
- Dyrbye LN, Satele D, West CP. Association of Characteristics of the Learning Environment and US Medical Student Burnout, Empathy, and Career Regret. JAMA Netw Open. 2021;4(8):e2119110. doi:10.1001/jamanetworkopen.2021.19110
- Ottesen A, Johansen M, Falkum E, et al. Shame in medical clerkship: “You just feel like dirt under someone’s shoe.” Perspect Med Educ. 2021;10:265-271. doi:10.1007/s40037-021-00665-w
- Norman S. The shame is not mine: addressing abuse of power dynamics in medical training. Int J Med Students. 2024;12(1). doi:10.5195/ijms.2024.2800
Jenna Mustafa is a third year medical student at the Hackensack Meridian School of Medicine. Her research focus has been on ethical dilemmas in clinical situations such as preserving dignity for patients who practice modesty, ethical military medicine, and pain pertaining to the opioid crisis.
Back to Table of Contents
|
| |
What Does "Advocacy" Look Like?
By: Gerald R. Stapleton
|
Working in health care, you recognize the mountains of challenges that people around you face every day of their lives. Sometimes it’s the disease they’re facing, sometimes it’s social, sometimes it’s bureaucracy, sometimes it’s financial, sometimes it’s the work environment, and sometimes it’s motivational. Facing these challenges alone can be hard. Sometimes an advocate can help, and often it takes a team of advocates to make a difference. You’ve seen it! You know it works!
The Academy for Professionalism in Health Care (APHC) will take an in-depth look at advocacy during the organization’s up-coming International Hybrid Conference titled “Professionalism and Advocacy - Achievements, Barriers and Complexities”. The conference will be held from June 3 -5, 2026 at Cooper Medical School of Rowan University (Camden, NJ) and via Zoom. In advance of the conference, we put out a call for everyone in the health care field to share images (e.g., photo, artwork, illustration, cartoon) that embody one’s perspective on the meaning or challenges of advocacy, and we have received a number of thought provoking submissions.
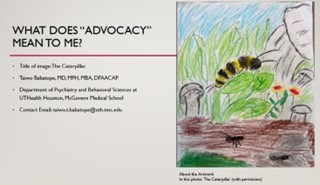
Taiwo Babatope, MD, MPH, MBA, DFAACAP from UT Health in Houston, shared an image titled “The Caterpillar” to convey various stages in the advocacy experience. In Taiwo’s words “The Caterpillar Stage represents vulnerability and misreading: A caterpillar is often misunderstood. People don't always recognize what it holds within it. For my patients, this stage reflects the moment when words are taken out of context — when others see surface behavior without understanding the neurological landscape beneath it.” The Cocoon, on the other hand, represents “the invisible, often painful work that happens between struggle and transformation. This is where our letters live — the spoken and written advocacy, the clinical explanation of diagnosis, the insistence that behaviors require support, not punishment. The cocoon is rarely seen by the outside world, but without it, there is no flight.” Meanwhile, “The Butterfly represents a return to the learning environment — but more than that, it represents a reclaimed identity. They return not as someone who had been forgiven, but as someone who had been understood. The butterfly doesn't hide its colors. It moves through the world in full view.”
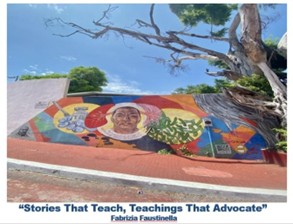
Fabrizia Faustinella, MD, PhD, MACP from the Baylor College of Health, captured a photo of a mural in a quaint uphill street in old town Acapulco that Fabrizia titled “Stories that Teach, Teachings that Advocate”. The mural tells the story of the fight against tuberculosis from the discovery of the mycobacterium to the BCG vaccine. It advocates for quality healthcare in the global fight against tuberculosis while also educating the community about how the disease is transmitted and the preventive role of vaccination.
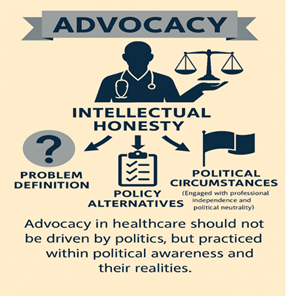
Stephen F. Gambescia, Phd, Med, MBA, MHum, MLS, MCHES from Drexel University took an innovative approach to creating his concept of advocacy. Stephen leveraged Microsoft Copilot with prompts that reflect the guidance he shares with his students when teaching about the public health policy making process. He asks his students to consider three streams of influence when creating policy, including a definition of the problem to be addressed, alternative policy solutions, and the political environment. His image stresses advocacy as the underlying goal, the three streams of influence just noted, and intellectual honesty as a balancing force that cuts across all of the considerations. He titled his image “Advocacy with Intellectual Honesty”.
Other submissions like one from Karla Williams from the AAMC have focused on the melding of self-advocacy and community advocacy coming together to serve deserving populations while others focus on communication as a form of advocacy. Participants in the upcoming conference on June 3 -5, 2026 at Cooper Medical School of Rowan University (Camden, NJ) and via Zoom will have the opportunity to see all of submissions from the “Images of Advocacy Collection” during conference activities.
And there is still time to share your ideas about what advocacy looks like!
Your image, for example, might reflect one of the critical themes to be discussed during the conference including:
- Who Needs Help - Patients, Learners, Providers, Systems?
- When to Advocate for Patients, Learners, Co-workers?
- Self-Advocacy – A Key to Wellness and Success for Patients, Learners and Professionals?
- Advocating for Justice and Peace – An Ethical Responsibility of Healthcare Professionals?
You can find some examples of images that are used to stimulate reflection on particular healthcare topics at Pulse Voices Visuals (https://pulsevoices.org/visuals/).
Submission Guidelines:
- Create an email titled “APHC advocacy image,” add the title of your image, your affiliation or location, and contact email in the text.
- Create a PowerPoint file to include: your selected Image, a title for your submission, your name, and the source and meaning of your image (if created with AI add the prompt used).
- Send your submission to Gerald Stapleton (Project Lead) at gstapltn@gmail.com.
- Submissions are due by Friday, May 15!
Submissions will be reviewed by Conference Committee members for relevance and creativity. Selected images will be exhibited on the APHC website, and during conference breaks. Conference participation is encouraged but not required to submit an entry.
By submitting your image, you acknowledge that we have the right to share the image and the accompanying text on the APHC website, in the organization’s newsletter, and during conference breaks. It is important that you have permission to use any copyrighted material or pictures of individuals identifiable in your submission.
Back to Table of Contents
|
|
|
Please join us on Friday, May 8, 2026, at 3 p.m. ET for APHC's Roundtable "Professionalism in Scholarship Leadership ."
This APHC Roundtable will explore Scholarship Leadership and ethics within this context as a core dimension of professionalism, with particular attention to how power dynamics and interests affect relationships between junior and established faculty and researchers, especially in authorship and mentoring relationships. The process of attaining the status of Scholarship Leadership will also be considered. The discussion will further address principles of transparent, contribution‑based authorship and the importance of early, open communication to promote fairness and trust. Furthermore, the culture of publishing, as well as the relationship between authors, reviewers, editors will be examined. Participants will also examine the growing influence of AI in scholarship, focusing on transparency, responsible use, and alignment with professional values. Overall, the roundtable will emphasize ethical scholarship leadership and how it depends not only on individual integrity but on institutional systems that support mentorship, accountability, and professional identity formation.
Our speakers:
Joshua Owolabi, MSc., MMedEd, MBA, PhD, PhD, FAcadMEd and
Mohamud Verjee, MD, MBA, CCFP, FCFP
🔎 Suggested reading pre-session:
Books: [1]. Boyer, E. L., Moser, D., Ream, T. C., & Braxton, J. M. (2016). Scholarship reconsidered: Priorities of the professoriate (Expanded ed.). Jossey-Bass. [2]. Owolabi, J. (2025). Technology enhanced medical and health education: A holistic approach. Routledge. Page 444- Why do people migrate into CoP?
Register at: https://tinyurl.com/2026Roundtables
Roundtables are for APHC Members only.
Check out our membership benefits here.
Join APHC to access previous Roundtable recordings.
Back to Table of Contents
|
Healthcare Professionalism: Education, Research & Resources Podcast
|
Professional Formation and APHC collaborate on a podcast, Healthcare Professionalism: Education, Research & Resources.
Over 125 podcast episodes have been released with over 17,000 downloads.
Released every other Saturday morning, recent episodes include Rachel Pittmann discussing Telehealth Etiquette and Amal Khidir talking about Designing the Faculty Development Professionalism Program with Multi-cultural Perspectives.
You can access the podcast episodes on your favorite platform or at: https://bit.ly/PF-APHC-Podcast
Back to Table of Contents
|
APHC Member Announcements
|
As a member, you have access to special benefits that include:
- Belonging to a community of like-minded professionals
- Participating in the monthly Professionalism Education
Roundtables with authors, faculty, and researchers, plus accessing past recordings
- Accessing 15 Professional Formation modules for individuals for free
- Enrolling in the APHC Faculty Development Certificate program known as LEEP (Leadership Excellence in Educating for Professionalism), which was launched in 2020 and offers longitudinal mentoring for a select group of
individuals seeking to deepen their knowledge and skills in
professionalism education, assessment, and research
- Posting your research, articles, podcasts, webinars, conferences, and books in the newsletter distributed to about 15,000 people
- Receiving a 20% discount on educational videos created by the Medical Professionalism Project, which also allows you to obtain MOC and CME
- Registering for APHC conferences with discounts
- Participating in APHC committees, which include the conference program, membership, and education committees
Our annual membership fees are very inexpensive and are valid for one year from the payment date. Select from seven types of membership, including the institutional membership for four people. See the descriptions.
Back to Table of Contents
|
The Academy Newsletter Editors
|
Editor-in-Chief: Bryan Pilkington | Managing Editor: Yvonne Kriss
Please contact Yvonne if you'd like to contribute an article to this newsletter.
If you know someone who would benefit from reading Professional Formation Update, please pass this along. They can subscribe to the newsletter by clicking here.
|
Academy for Professionalism in Health Care
PO Box 20031 | Scranton, PA 18502
|
Follow us on social media.
|
|